

The most used treatments in early ejaculation

- 4829
- 95
- Kristopher Greenholt
My goal with this article is not to stop in the theoretical aspects of premature ejaculation, but briefly contextualize the disorder to be able to carry out an eminently practical approach to the subject. Thus, the reader can get an idea of how this type of difficulties in the consultation of a psychologist are treated. If you want to deepen your theoretical conceptualization, the blog has already addressed the matter in this Article that talks about the most descriptive aspects of premature ejaculation.
Content
Toggle- What do we mean with premature ejaculation?
- Causes of early ejaculation
- Effective treatments
- 1. Compression and basilar squeeze (Masters & Johnson)
- 2. Stop and Start or Stop-Start (Semans)
- 3. Psychopharmacology
- Reflection
What do we mean with premature ejaculation?
As the name implies, this disorder is characterized by the presence of a orgasm and persistent or recurring ejaculation in response to minimal sexual stimulation before, for or a short time after penetration and in any case, before the person wishes. The most important thing to categorize it as a disorder, is that this dysfunction causes discomfort accused in the patient's life or difficulty in interpersonal relationships (eg. problems with your partner).
The usual thing in relation to the origin of the disorder is that the Male has learned this response in a defective way and normally in sexual situations where anxiety is present relevantly. Once the response has been learned, it is difficult to voluntarily control the reflection, since ejaculation depends on the sympathetic branch of the autonomic nervous system, directly related to the activation of the organism, so that the anxiety itself will help shoot the ejaculatory response.
Causes of early ejaculation
The vast majority of the sexual dysfunctions are from Psychosocial origin (Between 90 and 95% of cases, according to Kaplan, 1974, and Masters and Johnson, 1970). It has also been observed that they do not depend on a single exclusive cause but that multicausal models are usually formulated in its explanation. Although most of the dysfunctions respond to a psychosocial etiology, in some cases it is convenient to perform the relevant medical tests to rule out organicity.
Labrador in 1994, proposes three factors that are usually present in most sexual dysfunctions:
- Anxiety associated with sexual relations.
- Lack of skills and knowledge about him development of the answer sexual own and of the couple.
- Adoption of "Spectator role". This label refers to those people who are dedicated to ask, almost mechanically, if they will be doing well, if they will endure more than the previous time, if the other person will be liking, if the penis is hard enough, which It will be the next posture ... instead of just enjoying the sensations and experience. They become spectators of their own performance, instead of focusing on enjoying the game they are playing. In this way, much of our attention puts its focus on little or nothing relevant variables that will make it difficult to achieve a satisfactory sexual relationship for both parties.
The author adds, secondaryly, the importance of a Inadequate sex education, filled with sexual myths and mostly erroneous popular beliefs as relevant agents in the predisposition to sexual dysfunctions.
 Dysphasia: types, signs and treatment
Dysphasia: types, signs and treatment Effective treatments
1. Compression and basilar squeeze (Masters & Johnson)
As you can see, Masters & Johnson did not eat their heads with the name of this technique, but the most important thing for you is that this tool is an empirically effective resource, quite simple and that if it is constantly put into practice, it can provide you very positive results.
- First, get comfortable and relax.
- When you have achieved this state of calm and tranquility, it is when you can start to masturbate until a complete erection.
- The rhythm must be constant but with a moderate speed, until you feel that you are approaching the sensations that mark the moments before ejaculation.
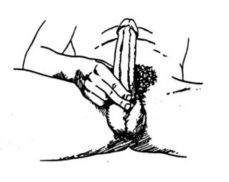
- When you reach this premonitory sensation, it is when you have to make a firm compression with the thumb on the frenulum and the index and medium fingers on the posterior face of the penis. The pressure must be strong (without painful) for three or four seconds, thus preventing the ejaculatory response. At this time, you will feel that your penis loses its ejaculatory urgency and your erection will decrease between 10 and 30%.
- It is convenient to rest between 15-30 seconds and after this brief period, you must restart the stimulation cycle until that feeling of imminent ejaculation again achieves again.
- In the first training sessions, it is convenient for you.
- Exercise should be practiced constantly until you perceive greater control over your ejaculatory response.

This training is usually done in 4 phases. Here we detail them as proposed by the Official College of Psychologists:
The first of them consists in performing the exercises described individually, As we have exposed or can also be one's own couple the one that stimulates and then exercises the pressure in the penis. For a correct application, the woman must be placed supported by the back of the head of the bed and with her legs stretched and open; The man rests on the back with his head directed towards the foot of the bed, his pelvis is placed between her legs. From that position the woman manipulates the genitals of men comfortably.
The second corresponds to the INTRODUCTION OF THE PENIS IN THE VAGINE WITHOUT MOVEMENT. In this case, the male will bed on their backs and the woman will be placed on top of him resting on the knees and surrounding the male with the legs. In this position the woman will introduce the penis into her vagina and keep it inside without making any movement while the male controls and prevents ejaculation. If the male notes that their excitation level endangers the control of ejaculation must immediately warn the woman and this after extracting the penis will apply the compression technique for 3 or 4 seconds. Once ejaculation retention is achieved, the woman will enter the penis again.
The third Consists of the INTRODUCTION OF THE PENIS IN THE VAGINA WITH MOVEMENT. Once the penis is introduced, the male will perform pelvic movements in order to maintain the erection, but without the ejaculation occurs, in the same position described in the previous step. In the event that the man feels the ejaculatory urgency, what will be done in the second phase will be repeated. Only when an adequate duration of penetration is achieved will be allowed ejaculation in this position.
In the quarter and last phase the intercourse It is done with a lateral posture, since it is the position that allows maximum control in ejaculation.
When you have achieved adequate control over ejaculation you can go to other positions, although it is usually recommended to avoid at the beginning those where the male is in a higher position (ex. Missionary Posture), since they hinder the control of ejaculation.
This process should be repeated until man learns to increase control over his ejaculation, first usually becomes individually and then accompanied by his partner, during intercourse, as we have developed.
You have to keep in mind that objective of this technique is not the immediate obtaining of pleasure, but with it the Reeducation of your ejaculatory reflex. If at any time you think you can ejaculate, it is necessary that you stop masturbating or that you take the penis of the vagina and do not get carried away by the sensations of pleasure, restarting the cycle that we expose here. This technique will allow you to more durable excitation response And so, you can directly stop the ejaculatory immediacy, fundamental characteristic of the premature ejaculation and center of your concerns. In this way you can prolong the time of permanence of the penis in the vagina without ejacular.
Masters & Johnson refer to the technique of Basilar squeeze as a variant we have just described. The main difference with the previous technique is that instead of compressing under the glans, the penis base is tightened.
2. Stop and Start or Stop-Start (Semans)
This time Semans also did not turn the name of the technique much, this greatly facilitates its explanation since the title itself is quite explicit.
The procedure is exactly the same as the one we have exposed in the previous technique and the main difference is that, in this case, no pressure exercise in the penis must be carried out when the man begins to feel that ejaculatory urgency. What should be done at this point is simply to stop stimulation, relax and restart the activity, once we have been able to control that excitation.
This technique has the same sequence as the previous one with what exactly runs through the same phases, explained by point by point in previous paragraphs.
3. Psychopharmacology
The last block of effective treatments consists mainly of the administration of SSRS (eg. fluoxetine) and tricyclic antidepressants (eg. clomipramine). They are usually paute when the behavioral techniques we have commented on in the previous paragraphs fail.
Reflection
One of the objectives of this article is to normalize early ejaculation, since I am aware that in our society it is lived, incomprehensibly for me, with great social stigma because values such as virility, masculinity and manhood are directly related to the power sexual.
It is convenient to know that it is the most prevalent sexual dysfunction in men, with figures of up to 27% and that usually occurs more frequently in young men and in the first sexual relations. This ailment can undermine, on many occasions, the self -esteem of a man, generate fears, insecurities, isolation, anxiety, blockages ... and it is necessary that whoever suffers it knows that he has Very good prognosis with adequate treatment. Authors such as Kilmann and Auerbach (1979) talk about a therapeutic success rate that is between 90 and 98%.
When you start a sexual relationship, you have to go from being an external spectator to a leading actor. You have to enjoy the movie and not dedicate yourself to attending to achievements or results. Focusing your attention on performance, the only thing you will favor is the appearance of anxiety and, with it, the consequent failure of the sexual response. Focus on your own sensations, since if you pay attention to irrelevant thoughts and other indications not related to the erotic keys of the situation, you have a great probability of confirming your concerns.
Your fear of failure will bring you directly to failure and the more expectations deposits in the process, you have the most probability of not fulfilling them. Break that vicious circle of concern-nerviosism-teens living the present moment.
If you are relaxed and focused on your contact with the other person, In the caresses, in the gestures .. You have many more possibilities of having a splendid and satisfactory sexual relationship. In this way, communication with your partner will also indirectly improve, an aspect that is usually central when working on most sexual dysfunctions. Eliminate taboos when talking about sex facilitates and improves experience significantly.
Definitely, worry less about how you are doing and enjoy more than you are doing. If you are not able to alone, do not hesitate to go to an expert to address it in a more effective, efficient and efficient way.
Kegel Exercises for men, benefits and commeraalize them