

Anorexia nervosa

- 4314
- 1057
- Lorenzo West I
Anorexia nervosa is one of the psychological disorders whose outcome can be death. In most cases the beginning of the disease usually coincides with that of adolescence. Although the age range has been varying throughout the history of the disease, the beginning of the disorder is between the ages of 14 and 18, being the risk strip between the age of 10 and 24, however today Cases are described in increasingly small girls, this data, together with the increase in pediatric age to 14 years, makes it a picture that can be detected from the pediatrician consultation.
Content
Toggle- Main characteristics of anorexia
- Anorexia subtypes
- Risk factors in anorexia
- Relatives:
- Personal:
- Social:
- Eating habits in anorexia
- Anorexia treatment
- Foster the basic principles of healthy eating behavior
Main characteristics of anorexia
The fundamental characteristic of anorexia nervosa It consists of a significant weight loss, below the minimum normal level, originated by the person himself, Through an exhaustive control of food intake, associated with intense fear of gaining weight and a serious distortion of its body image (dysmorphia), this weight loss is associated with a hormonal disorder that manifests itself in women as amenorrhea.
Weight loss is achieved through a decrease in total intake, ending in most cases with a very restricted diet, limited to a few foods. They change eating habits, obviate eating with more people, however they love to prepare meals with a high caloric degree so that others enjoy them. There are other ways of losing weight such as the use of self -trusted vomiting and the use of laxatives and diuretics (purges), as well as excessive exercise.
Anorexia subtypes
According to the diagnostic and statistical manual of the mental disorders DSM V, we can distinguish two subtypes in the nervous anorexia:
- Restrictive type: This subtype describes clinical pictures in which weight loss is achieved by diet, fasting or performing intense exercise. During anorexia nervous episodes, these people do not turn to binge or purges.
- Compulsive/purgative type: This subtype is used when the individual regularly resorts to binge and purges (or both). The majority of individuals who pass through the episodes of binge. There are some cases included in this subtype that do not have binge
resort to purges, even after ingesting small amounts of food.
 Stress and their relationship with diseases
Stress and their relationship with diseases Risk factors in anorexia
Relatives:
- Overprotection and rigidity. Interpersonal dependence.
- Stressful family environment.
- Normativity, Importance of social image and physical aspect.
- Obese relatives.
- Perfectionism, self-ex-expected and high expectations of achievement.
- Parents with addictive disorders (Bulimia), emotional or food.
Personal:
- Menarchy, excess weight, adult appearance.
- Significant people call "fat". Intense experiences of failure. Low tolerance to frustration.
- Perfectionism and self-ex-acence; High expectations of achievement and leave of self-efficacy. Execution anxiety.
- Perception of control loss; Fear of losing control. Feeling of impotence or dissatisfaction with itself.
- Self -control deficit.
- Fear of sexual maturity.
- Submissive or aggressive behavior; Social Skills Deficit.
Social:
- Importance of the physicist and social forms.
- Competitiveness, Perfectionism and achievement expectations.

Eating habits in anorexia
- Selective rejection of some foods
- Food handling (hide them, wash them, crumble them, remove fat and find a lot of waste)
- Development of obsessive-compulsive attitudes regarding food or drink (rituals, potomania)
- Isolation during meals or standing or moving
- Exaggerated food extension
- Alteration of food and sleep schedules
- Excessive interest in culinary issues
- Excessive attention to the intake of the rest of the family trying to make it abundant.
Different techniques and strategies are used to modify maladaptive eating behaviors. Stimulus control methods are normally used to control binge and purging behaviors in the Bulimia nervosa. He insist on the importance of making three meals a day, At the same time and in the same place, it serves to reduce the binge. In addition, the environmental stimuli that cause binge can be gradually extinguished through this method.
Anorexia treatment
Foster the basic principles of healthy eating behavior
- Make three meals a day
- Do not skip meals.
- Eating based on a consistent schedule. Never eat "career".
- Eaten
- Eat slowly
- Serve portions that go from moderate to small
- Do not buy food when you are hungry
- Do not use changes in weight to evaluate body image
- Establish behavioral objectives and adhere to them
Other procedures that encourage control over binge include teaching the patient to: Eat more slowly, throw smaller portions, leave food on the plate and throw out what is left over. It can also be useful to modify the choice of food and purchase practices, such as acquiring food when you are hungry. Behavioral contracts between the therapist and the patient can encourage adherence to food plans and specify behavioral objectives on the behavior of eating (P. Eg., Denign at a table at least five times a week or buy only ice cream instead of an ice cream bar). The use of reinforcement to increase the frequency of desirable food behaviors can increase the frequency of desirable food behaviors can increase adherence to the treatment program.
Gain weight is a treatment priority for anorexia nervosa. It has been found that the contingencies of the operant reinforcement constitute the effective method to increase the intake of calories in patients with internships (Benms, 1987). Negative consequences are programmed if the patient does not reach the objectives related to eating and gaining weight, such as privileges loss or intravenous feeding. In the modification of the eating habits of the anorexic, immediate feedback on the behavior of eating is required, accompanied by the positive and negative reinforcement consistent with the change in behavior. Behavioral contracts can be developed to facilitate the gradual increase in the frequency of healthy food behaviors, while encouraging a decrease in harmful eating behaviors. Exposure with response prevention. This procedure begins with the establishment by the therapist of an alliance with the patient and the explanation of the reasons and the treatment format.
Then, using the format that contains prohibited foods, A hierarchy of food is built that cause fear and anxiety. These feared foods are normally high in carbohydrates and/or fats, constitute foods ingested during binge and then, they are usually purged. Foods that cause less anxiety are exposed to the patient. In the presence of a therapist, the patient is avoided and encouraged to relax and what verbalize thoughts and feelings associated with eating food that fears. Patients also learn to attribute anxiety to erroneous cognitions instead of food. Exposure to eating normally 30 to 60 minutes. The desire to purify will generally disappear over a two -hour period. This format continues during several sessions and the patient is gradually encouraged to continue with the exposure of the food he fears, without the presence of the therapist, as a homework. Exhibition with response prevention is contemplated as a election procedure (Rosen and Leitenberg, 1982). Pur was considered as an escape response to the fear and anxiety of gaining weight.
A version of the "is currently recommendedExhibition with response prevention"More similar to live desensitization than to the flood method initially written by Rosen and other colleagues (Williamson" Barkery Norris, 1993).
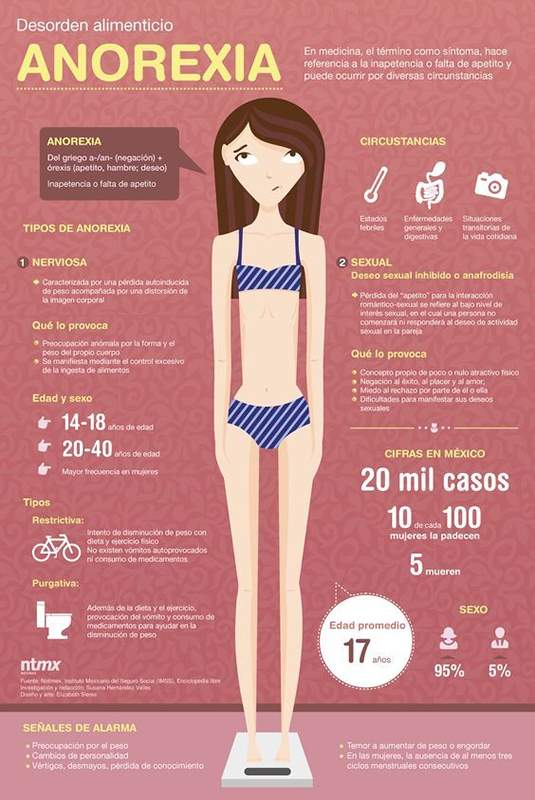
As an image says more than a thousand words, then we present an infographic about anorexia:
- « Mental techniques to combat stress
- Differences and similarities between the evolutionary theory of Piaget and Vygotsky »